


Clinical Case – Zygomatic Implants | 1
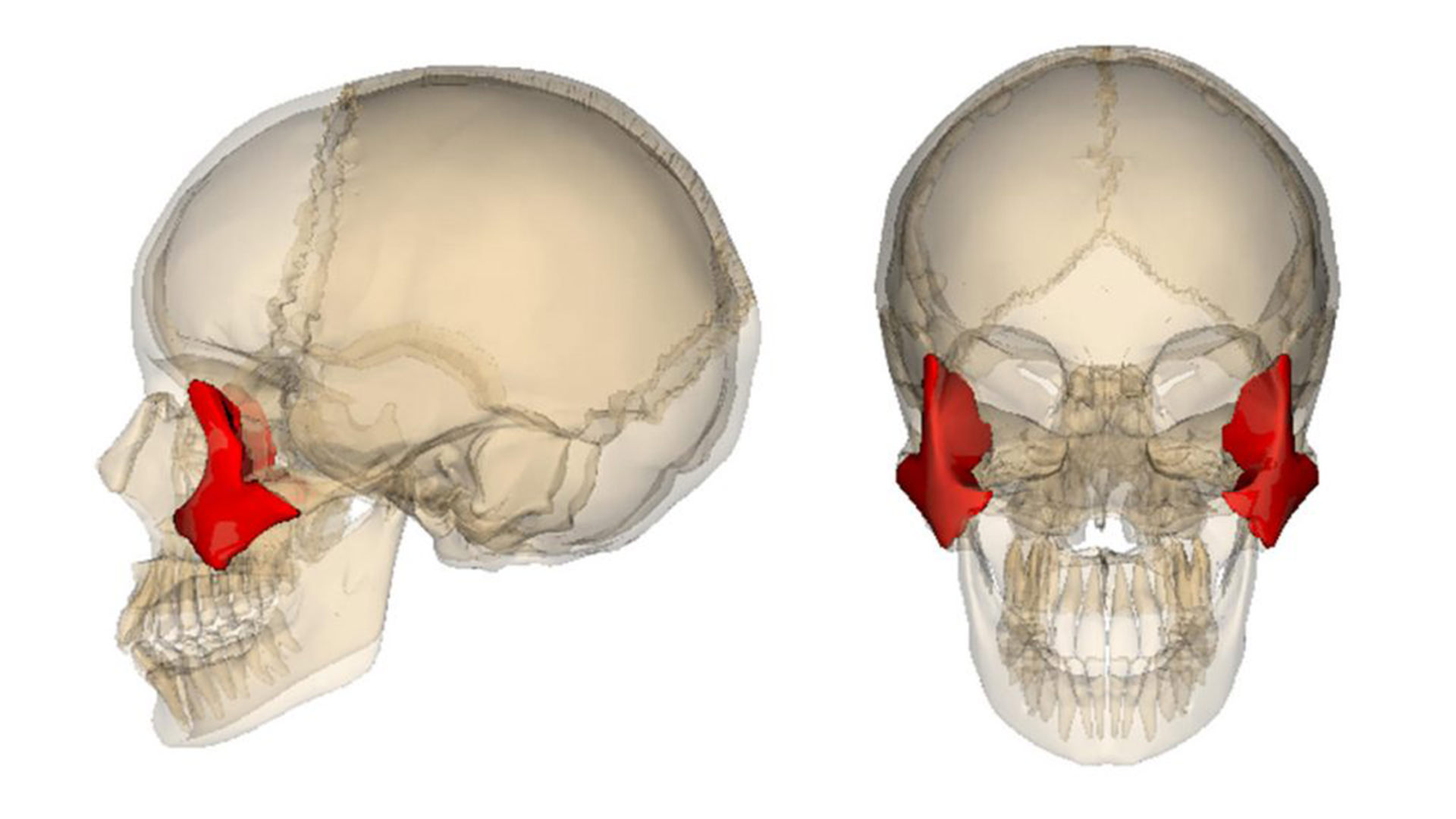
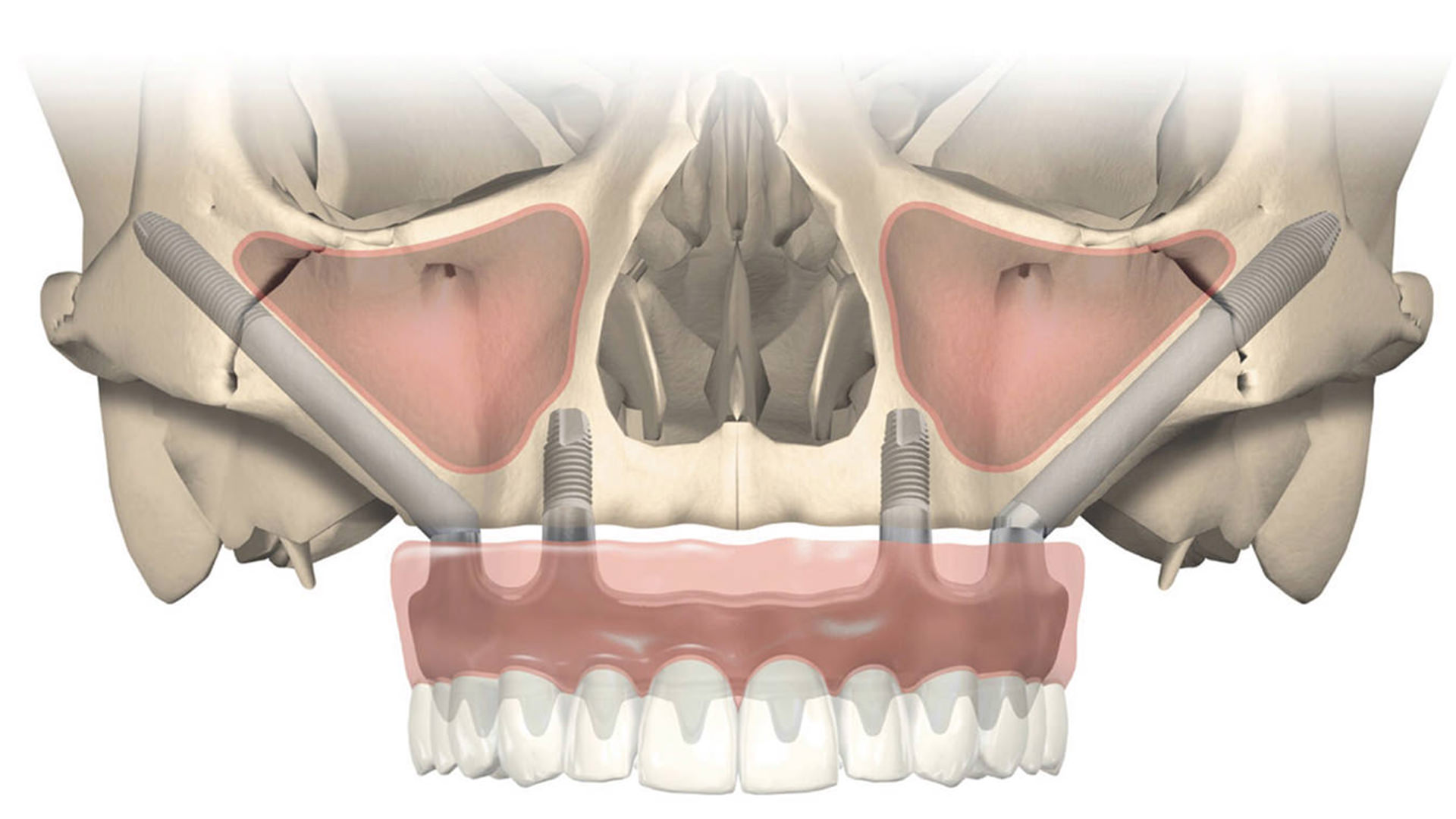
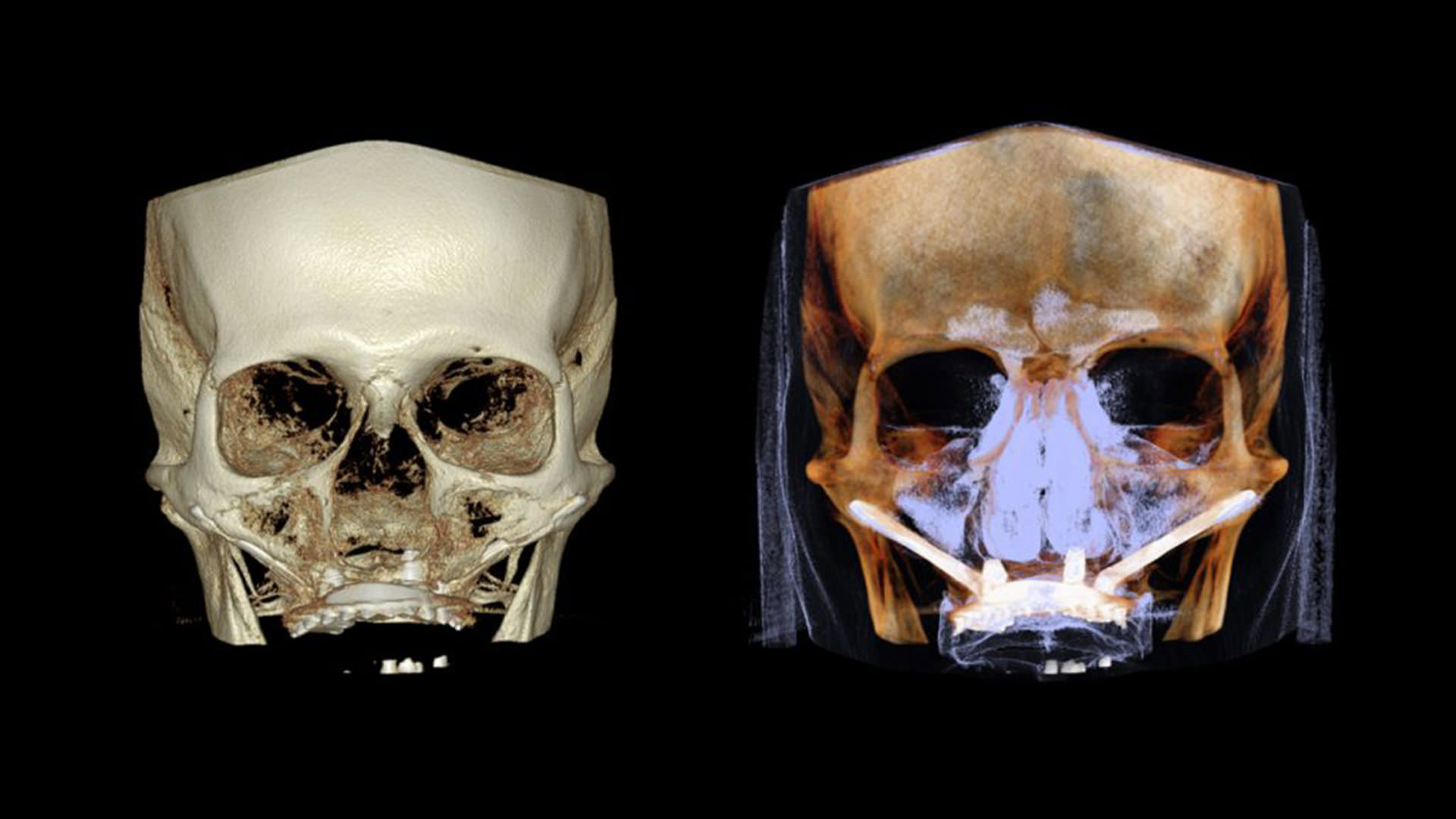
Zygomatic Implants 66 years old Estoril Zygomatic implants This is a technique for patients with severe and extreme resorption of the upper jaw who wear

Clinical Case – Zygomatic Implants | 2
Zygomatic implants 49 anos Belgium Zygomatic implants This is a technique for patients with severe and extreme resorption of the upper jaw who wear full

Clinical Case – Zygomatic Implants | 4
Zygomatic Implants 59 years old Cascais Zygomatic implants This is a technique for patients with severe and extreme resorption of the upper jaw who wear